AtaGenix Laboratories

AtaGenix Laboratories
Release time: 2026-01-14 View volume: 1072
Project Snapshot — A Cancer Communications study mapped a pAKT–pPCK1–pLDHA–SPRINGlac axis that rewires mevalonate flux to block ferroptosis and drive chemo-immunotherapy resistance in AKT-hyperactivated intrahepatic cholangiocarcinoma (ICC). Simvastatin disrupted this axis and restored therapy sensitivity in preclinical models. AtaGenix provided the two custom phospho-specific antibodies (anti-pPCK1 Ser90, anti-pLDHA Thr248) that enabled direct readout of axis activation status.
Based on: Zhu J et al., Cancer Communications, 2025;45(8):1038–1071 — DOI: 10.1002/cac2.70036
Intrahepatic cholangiocarcinoma (ICC) is an aggressive malignancy with a 10% 5-year survival rate across all stages, dropping to 3% in distant-stage disease. While chemo-immunotherapy (gemcitabine/cisplatin + anti-PD-L1) has become a new standard following TOPAZ-1 and KEYNOTE-966, resistance remains common. AKT hyperactivation is prevalent across many tumors, raising a central question: how does AKT-driven metabolism protect tumor cells from immunotherapy-augmented killing?
Using in vivo metabolic CRISPR screening in a KrasG12D/Tp53−/− ICC mouse model under chemo-immunotherapy, the authors identified phosphoenolpyruvate carboxykinase 1 (PCK1) as a key ferroptosis resistance driver and mapped a mechanistic cascade connecting AKT signaling to mevalonate pathway flux. Critically, simvastatin (a mevalonate pathway inhibitor) augmented chemo-immunotherapy efficacy in preclinical models, and pAKT–pPCK1 emerged as a biomarker candidate for patient stratification.
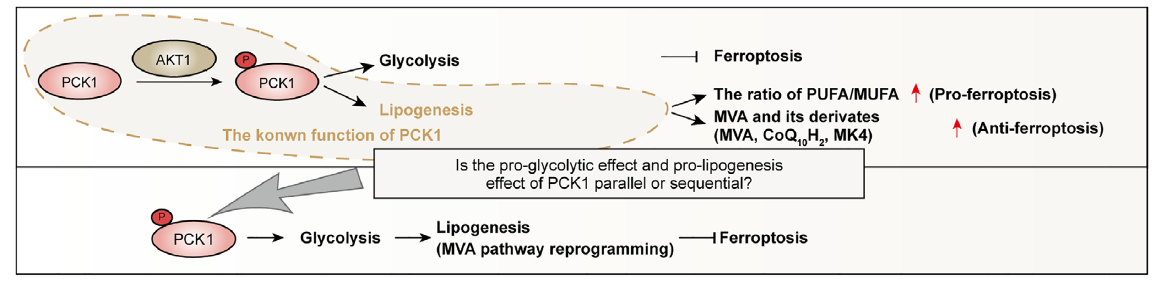
Fig. 1. Validation of pPCK1-mediated ferroptosis resistance. AKT phosphorylates PCK1 at Ser90, driving mevalonate flux and antioxidant shielding. Adapted from Zhu et al., Cancer Commun 2025.
1. Signal Initiation: AKT phosphorylates PCK1 at Ser90 (pPCK1), establishing an AKT-dependent metabolic state less permissive to ferroptosis.
2. Metabolic Coupling: pPCK1 increases flux through the mevalonate pathway, enhancing synthesis of radical-scavenging metabolites including ubiquinol (CoQ10H2) and menaquinone-4 (MK4).
3. Axis Execution: The cascade operates through the pPCK1–pLDHA–SPRINGlac axis, linking lactate metabolism, post-translational modification, and mevalonate activation.
4. Functional Consequence: Elevated antioxidant capacity suppresses lipid peroxidation, enabling ICC cells to survive chemo-immunotherapy pressure in AKT-hyperactivated contexts.
Interfering with the mevalonate pathway using simvastatin significantly enhanced chemo-immunotherapy efficacy in preclinical ICC models by disrupting the axis-linked antioxidant shield. The therapeutic logic: block mevalonate flux → reduce antioxidant buffering → restore lipid peroxidation → re-enable ferroptosis under therapy. This frames AKT-hyperactivated ICC as a tumor subtype with a druggable metabolic dependency.
If AKT-driven pPCK1 activation is a prerequisite for mevalonate-mediated ferroptosis resistance, then tumors with elevated pAKT and pPCK1 may represent a subgroup with distinct resistance biology — and a distinct opportunity for combination strategies targeting the axis. The paper reports clinical relevance for pPCK1 in AKT-hyperactivated ICC patients receiving chemo-immunotherapy, supporting pAKT–pPCK1 as a predictive biomarker candidate.
Phospho-Site Specificity: Custom antibodies recognizing pPCK1 (Ser90) and pLDHA (Thr248) enable direct readout of axis ON/OFF states, rather than indirect pathway inference.
Mechanistic Validation: Integrated into IP–WB workflows including phospho-peptide mapping and interaction-focused assays to connect phosphorylation events with downstream functional consequences.
Translational Readiness: Phospho-marker quantification in tissue contexts supports biomarker exploration and patient stratification hypotheses around pAKT–pPCK1.
QC Rigor: Phospho-peptide design with negative selection against non-phosphorylated peptides, and application-specific validation (WB/IP/IHC) to minimize off-target signal.
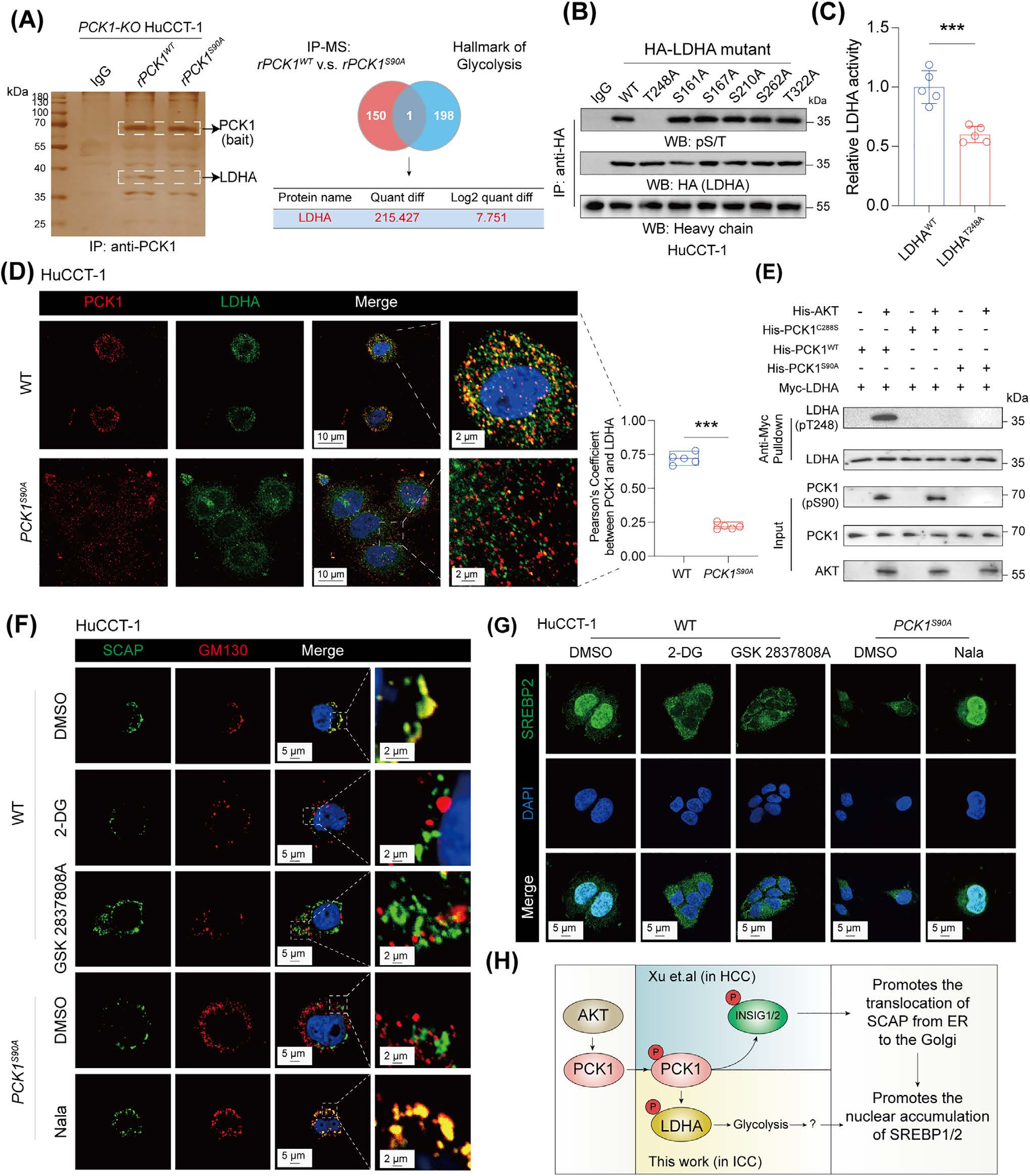
Fig. 2. Detection results of AtaGenix custom phospho-antibodies: anti-PCK1 pS90 and anti-LDHA pT248 in ICC cell lysates. Adapted from Zhu et al., Cancer Commun 2025.
2
Custom Phospho-Antibodies
pPCK1 + pLDHA
Phospho-Sites Targeted
WB/IP/IHC
Validated Applications
ICC
Disease Model
Why This Matters
This study establishes the pAKT–pPCK1–pLDHA–SPRINGlac axis as a mechanistic driver of ferroptosis resistance and chemo-immunotherapy resistance in AKT-hyperactivated ICC. It provides both a drugging concept (simvastatin-based mevalonate interference) and a biomarker concept (pAKT–pPCK1 for patient stratification). AtaGenix's custom phospho-antibodies (pPCK1 Ser90, pLDHA Thr248) were essential for high-fidelity detection of the key mechanistic nodes — tools that did not exist commercially and were built de novo for this translational research program.
1. Zhu J, Xiong Y, Zhang Y, et al. Cancer Communications. 2025;45(8):1038–1071. DOI: 10.1002/cac2.70036
2. Oh D-Y, et al. TOPAZ-1. NEJM Evidence. 2022. DOI: 10.1056/EVIDoa2200015
3. Kelley RK, et al. KEYNOTE-966. The Lancet. 2023.
For research use only. This page provides scientific literature interpretation and does not constitute medical advice or treatment recommendations.
Need custom phospho-specific antibodies for signaling axis validation, biomarker exploration, or translational assay development? AtaGenix delivers site-specific phospho-antibody programs with rigorous epitope design and multi-application validation.
Talk to Technical SupportResponse within 24 hours
Contact Us
+86-27-65523339
info@atagenix.com
Building C, R & D Building, No. 666, Shendun 4th Road, Donghu New Technology Development Zone, Wuhan
